UNTWINING THE TWINDEMIC
The world today is under the clutch of a “Twindemic” of vitamin D deficiency and COVID-19. A twindemic is a portmanteau of “Twin” and “Pandemic”. Vitamin D deficiency is considerably under-diagnosed, and under-treated nutritional deficiency that is more pandemic than the Coronavirus today. A growing volume of research is uncovering a synergistic association between insufficient sunshine vitamin levels and COVID-19 infectivity. British researchers have reported a connection between low levels of vitamin D and high numbers of COVID-19 cases and mortality rates across 20 European nations.
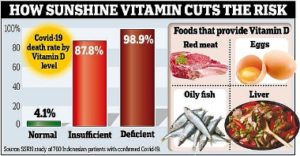
 Recently, some studies have emerged that are tying vitamin D deficiency with an increased risk of mortality from COVID-19. The Northwestern University research team analysed the data from hospitals across China, France, Germany, Italy, Iran, South Korea, Spain, Switzerland, the United Kingdom (UK) and the United States. It noted high mortality rates in countries such as Italy, Spain and the UK that had lower levels of vitamin D in their communities compared to countries which were less severely affected. The data from around the globe disclosed a strong correlation of vitamin D levels with cytokine storm and mortality. Countries like Spain and Italy, though reasonably sunny, experienced the highest infection and fatality rates in the world when compared to low casualty rates in Nordic countries like Norway, Finland and Sweden despite meagre sunlight exposure because of fortification of foods with vitamin D and high consumption of vitamin D supplements. Further, a study in Spain revealed that more than 80 % of patients who were tested positive for coronavirus were vitamin D deficient. In contrast, another study uncovered that COVID-19 patients who had adequate vitamin D levels had a 51.5 percent lower risk of dying from the disease.
Recently, some studies have emerged that are tying vitamin D deficiency with an increased risk of mortality from COVID-19. The Northwestern University research team analysed the data from hospitals across China, France, Germany, Italy, Iran, South Korea, Spain, Switzerland, the United Kingdom (UK) and the United States. It noted high mortality rates in countries such as Italy, Spain and the UK that had lower levels of vitamin D in their communities compared to countries which were less severely affected. The data from around the globe disclosed a strong correlation of vitamin D levels with cytokine storm and mortality. Countries like Spain and Italy, though reasonably sunny, experienced the highest infection and fatality rates in the world when compared to low casualty rates in Nordic countries like Norway, Finland and Sweden despite meagre sunlight exposure because of fortification of foods with vitamin D and high consumption of vitamin D supplements. Further, a study in Spain revealed that more than 80 % of patients who were tested positive for coronavirus were vitamin D deficient. In contrast, another study uncovered that COVID-19 patients who had adequate vitamin D levels had a 51.5 percent lower risk of dying from the disease.
Further, people having black skin were more affected by vitamin D deficiency because of the presence of melanin pigment, which prevents UV light from rapidly acting on the skin. Out of 15,000 Covid 19 patients admitted to American hospitals, 33% of them were black Americans. Despite blacks making only 13% of the general population. 40% of Covid 19 patients who died in a hospital in Stockholm, Sweden were of Somalia origin. This is even though the percentage of Somalis living in the area was only 0.84%. When healthy men and women older than the age of 65 in Boston were surveyed for Vitamin D status, a surprising 34% of white, 42% of Hispanic and a vast 84% of African American men were vitamin D deficient.
Vitamin D Figure Color
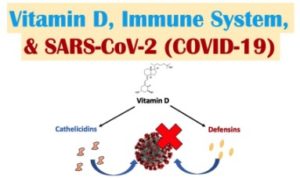
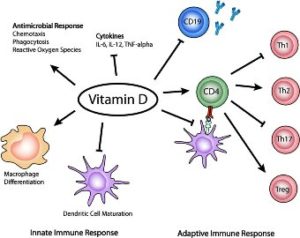
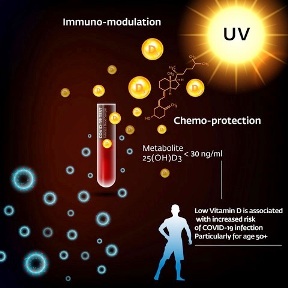
Vitamin D gets synthesised endogenously when the skin gets exposed to sunlight. Investigators have discovered three ways by which vitamin D deficiency predisposes humankind to COVID-19 pandemic. First, vitamin D inadequacy makes people susceptible to COVID-19 by modifying the Renin-Angiotensin” System, and eliciting the deadly ”cytokine storm”. Second, the people who are easily vulnerable to severe vitamin D deficiency such as older men, ethnic groups with skin rich in melanin, the obese, and people with comorbidities are at the highest peril of COVID afflictions. And third, the pattern of the geographical spread of COVID-19 reflects higher population vitamin D deficiency.
COVID-19 infection commences when the virus enters the body through ACE2 receptors in the nose, as they are plentiful there. From there, the virus may advance and infiltrate cells at other places such as intestines, kidneys and heart, which also possess ACE2 receptors. After infecting the cells, the virus hijacks the body’s systems. It up-regulates ACE2 receptors, which in turn tweaks the renin-angiotensin system (RAS). It wrests control over the body’s production of a chemical called bradykinin and incites it to go to topsy-turvy. Because of the coronavirus infection, ACE receptors become inefficient at tearing down bradykinin, causing it to accumulate and snowball into a bradykinin storm which accounts for many deadly effects of COVID-19. Besides, the ACE2 receptor, dipeptidyl peptidase-4 receptor (DPP-4/CD26) is the second usable access route. Administration of vitamin D drastically dwindles the chances of infection by modification of both the access routes.
 Vitamin D deficiency is globally prevalent among all age groups, especially at high latitudes > 40° as insignificant UV-B radiations reach the earth’s surface during winters. Although India is close to the equator and receives a substantial quantity of sunlight throughout the year, most of the Indian population (50–90%) is deficient in vitamin D. Besides, as exceptional rates of COVID-19 infection and mortality seemed off-kilter in various states, and Union Territories of India, Sunali Padhi and her co-workers embarked on a first of its kind study to investigate the association of vitamin D with COVID-19 infection and mortality rates in the Indian population. In September 2020, the group published the findings of their research, which affirmed a significant association of lower levels of vitamin D with COVID-19 related deaths and susceptibility to infection.
Vitamin D deficiency is globally prevalent among all age groups, especially at high latitudes > 40° as insignificant UV-B radiations reach the earth’s surface during winters. Although India is close to the equator and receives a substantial quantity of sunlight throughout the year, most of the Indian population (50–90%) is deficient in vitamin D. Besides, as exceptional rates of COVID-19 infection and mortality seemed off-kilter in various states, and Union Territories of India, Sunali Padhi and her co-workers embarked on a first of its kind study to investigate the association of vitamin D with COVID-19 infection and mortality rates in the Indian population. In September 2020, the group published the findings of their research, which affirmed a significant association of lower levels of vitamin D with COVID-19 related deaths and susceptibility to infection.
 Likewise, Linda Benskin, an independent researcher, published a paper in the September 2020 issue of ”Frontiers in Public Health” where she reviewed the original research studies that showed an association between serum vitamin D levels and COVID-19 risk through an exhaustive literature search performed on PubMed, Google Scholar, and RSMLDS. In the paper, she stressed 141 published articles that had documented the plausibility of vitamin D deficiency playing a part in infection and advancement of COVID-19 disease. She also summarised 47 original research studies that had proclaimed correlation and causal evidence for the assumption that vitamin D deficiency was a causal component in COVID-19 outcomes. The literature review also divulged that it would be prophylactically feasible to correct vitamin D deficiency by administering a daily dose of 2000 IU vitamin D to the at-risk populations despite the non-existence of official government policies in most countries including India to favour vitamin D supplementation to lessen COVID-19 risk and severity. This one small step within safe thresholds has the potential to diminish COVID-19 fatalities all over the world dramatically.
Likewise, Linda Benskin, an independent researcher, published a paper in the September 2020 issue of ”Frontiers in Public Health” where she reviewed the original research studies that showed an association between serum vitamin D levels and COVID-19 risk through an exhaustive literature search performed on PubMed, Google Scholar, and RSMLDS. In the paper, she stressed 141 published articles that had documented the plausibility of vitamin D deficiency playing a part in infection and advancement of COVID-19 disease. She also summarised 47 original research studies that had proclaimed correlation and causal evidence for the assumption that vitamin D deficiency was a causal component in COVID-19 outcomes. The literature review also divulged that it would be prophylactically feasible to correct vitamin D deficiency by administering a daily dose of 2000 IU vitamin D to the at-risk populations despite the non-existence of official government policies in most countries including India to favour vitamin D supplementation to lessen COVID-19 risk and severity. This one small step within safe thresholds has the potential to diminish COVID-19 fatalities all over the world dramatically.
To tackle the vitamin D deficiency epidemic in India, a population-based approach such as food fortification could yield better results than vitamin D supplementation. Several advanced nations have launched nationwide milk fortification programs to improve vitamin D status. In India, fortified milk is being sold in Delhi, Jharkhand and few other states. Fortification of staple foods is not a novel concept. In 1976, consumption of fortified chapati flour by people of Indian origin in the UK helped immensely in raising serum vitamin D levels significantly. To improve vitamin D levels in our state, we could contemplate adding vitamin D to milk, yoghurt, ghee, wheat flour, maida, rice/ rice flour and various premixes available in stores for idli, dosa, uthappam, etc. By doing so, we could achieve a significant overall improvement in vitamin D levels in our state.
 The Department of Homeland Security has shown that sunlight is a double-edged sword as it not only kills the COVID-19 virus swiftly but also prevents the proliferation of the virus inside the body and stops its transmission outside the body. Sunlight produces 20000 IU of vitamin D in the human skin from 20-minute exposure to the sun during the mid-day. This accounts for approximately 90% of our total vitamin D, with only 10% coming from food. Published research reveals that late morning sun (between 11 am to 1 pm) is the most beneficial time for human skin to synthesise vitamin D. In the Directorate of Vigilance, I have issued an advisory to the staff to spend at least half-hour outside the office on the terrace and under the sun during the lunch break. A similar initiative could be contemplated in the entire state to boost vitamin D levels in the whole population. Achieving vitamin D sufficiency in the community through sunlight exposure could result in savings of several thousand crores of rupees in terms of reduction of health costs and savings.
The Department of Homeland Security has shown that sunlight is a double-edged sword as it not only kills the COVID-19 virus swiftly but also prevents the proliferation of the virus inside the body and stops its transmission outside the body. Sunlight produces 20000 IU of vitamin D in the human skin from 20-minute exposure to the sun during the mid-day. This accounts for approximately 90% of our total vitamin D, with only 10% coming from food. Published research reveals that late morning sun (between 11 am to 1 pm) is the most beneficial time for human skin to synthesise vitamin D. In the Directorate of Vigilance, I have issued an advisory to the staff to spend at least half-hour outside the office on the terrace and under the sun during the lunch break. A similar initiative could be contemplated in the entire state to boost vitamin D levels in the whole population. Achieving vitamin D sufficiency in the community through sunlight exposure could result in savings of several thousand crores of rupees in terms of reduction of health costs and savings.
During the “Spanish flu” pandemic of 1918-1919, doctors could substantially decrease deaths when patients were treated in “open-air” hospitals with access to sunlight, because of suppression of “cytokine storm” by vitamin D.
Besides, sunlight cures several diseases, including heart disease through nitric oxide production, it improves mood through serotonin production and also helps reset the circadian rhythm. The short story ” Sun” written by D.H.Lawrence in 1925 tells the story of a doctor prescribing Sun exposure to Juliet, a middle-class matron who travels to Sicily where she is healed and made whole again.
Finally, if restoration of the deficiency of vitamin D levels in the community could usher better COVID-19 outcomes then likewise on the spiritual plane, amelioration of the spiritual poverty in the world through inner work and cultivation of higher consciousness could heal this planet from the twindemic of social turmoil and conflict that is ripping apart the social fabric of our society?
Source from: epaper/dtnext/chennai/dt:22.11.2020
 Dr.K. Jayanth Murali is an IPS Officer belonging to 1991 batch. He is borne on Tamil Nadu cadre. He lives with his family in Chennai, India. He is currently serving the Government of Tamil Nadu as Director / Additional Director General of Police, Vigilance and Anti-Corruption.
Dr.K. Jayanth Murali is an IPS Officer belonging to 1991 batch. He is borne on Tamil Nadu cadre. He lives with his family in Chennai, India. He is currently serving the Government of Tamil Nadu as Director / Additional Director General of Police, Vigilance and Anti-Corruption.

